
It is 9:14pm on a Tuesday. A parent in Hamilton has a feverish toddler and wants the first appointment tomorrow. Your line rolls to an answering machine. They hang up, ring the practice down the road, and book there instead.
A medical answering service after hours is the difference between catching that patient and donating them to a competitor. Most clinics still treat the hours after 5pm as dead air. They are not. They are the busiest enrolment window you are ignoring.
This runs on the same platform that answers your clinic phones around the clock. This article is only about the after-hours slice of it.

After 5pm the desk is empty, but the phone keeps ringing with bookings.
What happens to your clinic calls after 5pm?
After 5pm your booking line usually rolls to voicemail, and most patients never leave a message. They simply hang up and dial the next clinic. A clinic taking 40 evening calls a week loses a real slice of new enrolments to whoever answers first. That is revenue walking out in silence.
Watch your own after-hours log for a week. You will see the same pattern in every NZ and AU practice. Calls cluster between 6pm and 9pm, when working parents finally sit down.
They are not emergencies. They are bookings, reschedules, and repeat script requests that your daytime team would happily handle.
The problem is timing, not demand. Your reception team has gone home. The patient has not gone away. They have just moved their problem to a competitor who picked up.
We covered the daytime version of this in our piece on ending the 8am redial scramble at a clinic. This article is about the other end of the clock. The hours when nobody is at the desk and the phone still rings.
What does an after-hours medical answering service do?
An after-hours medical answering service answers every evening and weekend call instantly, books or reschedules appointments, takes repeat prescription requests, and answers routine questions about hours and enrolment. Urgent calls get flagged and escalated to a person. The agent never gives clinical advice. It captures, books, and routes.
Think of it as your front desk, awake at 8pm. The agent picks up in under a second, greets the caller, and discloses up front that they are speaking with an AI assistant. Then it does the boring, valuable work your voicemail cannot.
It books a new patient into a free slot. It moves tomorrow's 10am to Thursday. It logs a repeat prescription request for the nurse to action in the morning.
Everything it handles lands in a morning summary. Your practice manager reads one tidy list at 8am instead of fishing through twelve voicemails. Nothing gets lost, and nobody got woken up.
This is the overflow pattern, not a replacement for your team. The same approach works across trades and clinics. We explain the broader version in our guide to running an after-hours receptionist. The clinic version just has tighter rules about what the agent can say.
Every evening call sorts into book, reschedule, repeat script, or escalate.
How does it book and triage without giving clinical advice?
The agent books and reschedules by reading your live availability and writing the booking straight back. It triages by sorting calls into routine and urgent, using plain rules you set. It never assesses symptoms or suggests treatment. When a caller describes something clinical, the agent collects details and routes. It does not diagnose.
Here is the line we hold. Booking is administrative. Triage, in our build, means routing, not clinical judgement.
The agent asks structured questions to decide who needs a person tonight and who can wait for the morning. It does not tell anyone whether their chest pain is serious.
A caller wanting a routine appointment gets booked. A caller asking to reschedule gets moved. A caller mentioning anything urgent gets the escalation path, fast.
Software that books is administrative. Software that advises is clinical, and we do not build that. Our appointment booking agent for NZ and AU clinics handles the booking half cleanly and leaves the clinical calls to clinicians.
We are also honest that not every call should be handled by software. Some need a human, immediately. We wrote about exactly where that line sits in our piece on why voice agents still need humans.
How does it keep patient data inside the Privacy Code and APPs?
Patient data is collected on a minimisation basis, stored in our Sydney data centre, and handled under the NZ Health Information Privacy Code 2020 and the Australian Privacy Principles. The agent asks only for what a booking needs. It discloses it is an AI. Sensitive health detail is kept to the minimum required to route the call.
Let us be precise about where data lives, because honesty here is the whole point. Your portal, your transcripts, and your structured call records sit on our servers in Sydney. The live audio of the call itself is processed offshore in real time.
We will never tell you all your data stays in Australia, because the voice runtime does not.
For a New Zealand clinic, the rules come from the Health Information Privacy Code 2020, overseen by the Office of the Privacy Commissioner. For an Australian practice, it is the 13 Australian Privacy Principles under the Privacy Act 1988, overseen by the OAIC.
One important clarification. HIPAA is United States law. It does not apply to a clinic in Tauranga or Toowoomba, and any vendor citing HIPAA at you is selling the wrong map.
We minimise what the agent asks for. A booking needs a name, a contact number, a reason category, and a preferred time. It does not need a full clinical history, so the agent does not collect one. Less data captured is less data to protect.
If you want the deeper read on how a voice agent sits inside the NZ Privacy Act 2020, we wrote a dedicated breakdown. For the clinic-specific security view, our healthcare security page lays out the buyer-side outcomes in plain English.
Worried about patient data after hours?
Our healthcare voice agent overview shows exactly what the agent collects, where it sits, and what it refuses to touch.
When does it escalate an urgent call to a person?
The agent escalates the moment a call matches an urgent rule you define, transferring to your on-call number or after-hours service. You set the triggers. Anything that sounds like a medical emergency, a distressed caller, or a request the agent cannot resolve gets a person, not a booking slot. Escalation is the default when in doubt.
You write the escalation rules during setup. A typical clinic routes emergencies to 111 in New Zealand or 000 in Australia. It routes after-hours clinical concerns to the on-call GP or your contracted line. The agent reads from your rules, not its own judgement.
Picture a 7pm call from someone short of breath. The agent does not book them for Thursday. It recognises the urgent trigger, gives the emergency instruction, and routes immediately.
That single correct escalation is worth more than a hundred tidy bookings. The agent is tuned to escalate generously. A false escalation costs a few seconds of a human's time. A missed one costs far more.
You pay for minutes talked, not a fixed evening roster.
What does after-hours cover cost a NZ or AU practice?
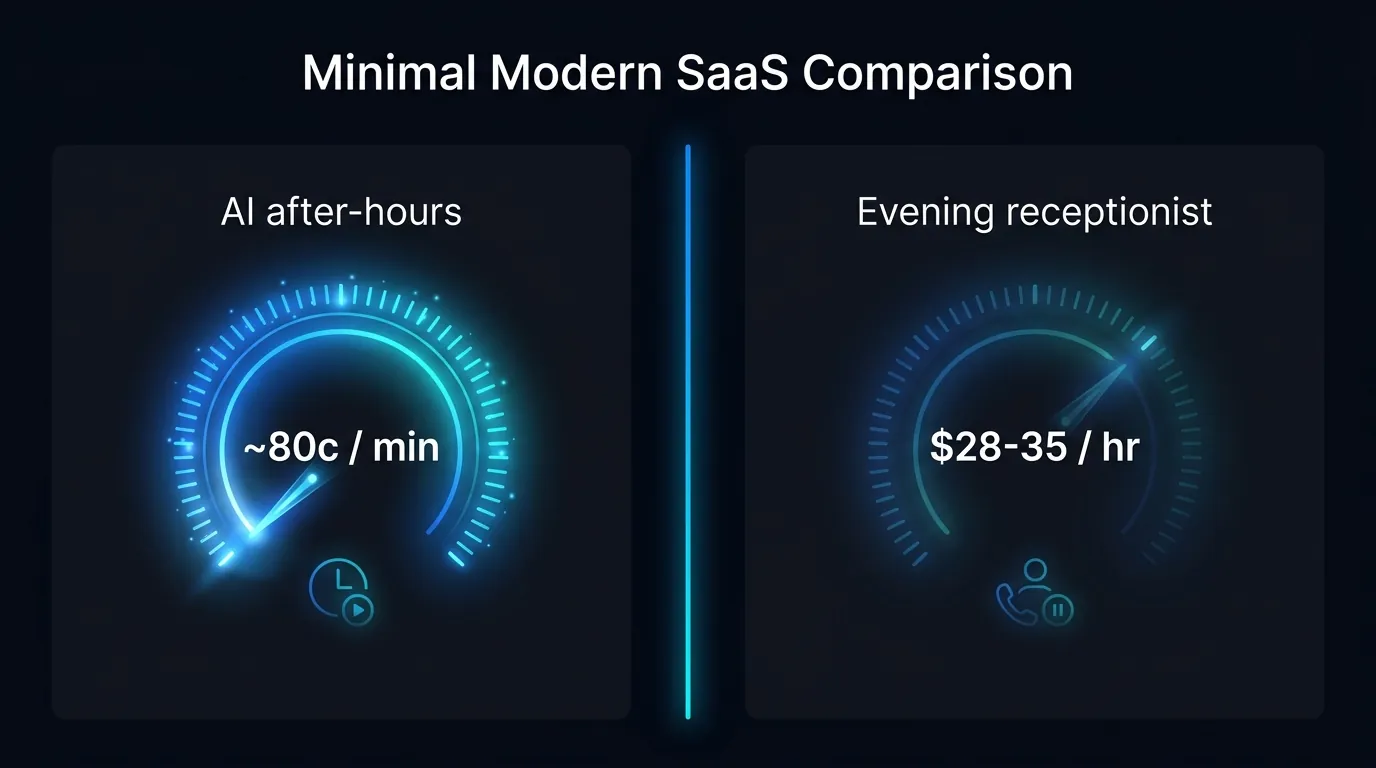
After-hours cover runs at about 80 cents per minute in NZD or AUD, billed by the second. A typical answered call lasts around 30 seconds, so roughly 40 cents. A one to two minute booking costs about one to two dollars. There is no hourly wage, no holiday pay, and no KiwiSaver or super on top.
Compare that to staffing the evenings with a person. A part-time receptionist in New Zealand or Australia costs roughly $28 to $35 an hour before KiwiSaver or super, ACC, and holiday pay. Three hours of evening cover, five nights a week, is a real line item.
Run the maths on your own diary. If after-hours cover catches even three new enrolments a month that would otherwise have rung a competitor, the bill is paid back several times over.
You only pay for conversations that happen. A quiet Sunday costs almost nothing. A busy Monday evening costs a few dollars. The cost scales with the calls, not with a fixed roster.
Does it work with your practice management system?
In most cases, yes. The agent books into your existing availability and writes the appointment back so your front desk sees it the next morning like any other booking. Where a direct connection is not yet available, the agent captures the full booking and drops it into your morning summary for one-tap confirmation. Either way, nothing is lost.
We scope the integration during setup. The goal is that an evening booking shows up in your system the same way a daytime one does, with no double entry. Your team should not be able to tell whether a human or the agent took the booking.
Start with after-hours overflow if you want the lowest-risk first step. The agent handles only the calls your voicemail currently swallows. Your daytime workflow does not change at all, and you review the results each morning before trusting it further.
From there, most clinics extend the same agent to daytime overflow and the 8am rush. The build for medical clinics is designed to grow from a cautious evening pilot into full-day cover at your pace.
Stop donating your 9pm callers to the clinic down the road.
See how our after-hours medical answering build handles booking and triage without ever giving clinical advice.
Frequently Asked Questions
Does the after-hours agent tell patients it is an AI?
Yes, on every call. The agent discloses up front that the caller is speaking with an AI assistant before it takes any details. This is both good practice and the honest thing to do. Patients consistently keep talking once they know it can actually book them in tonight rather than leave them on hold.
Can the agent give medical advice if a patient is worried?
No, and that is deliberate. The agent never assesses symptoms or suggests treatment. If a caller raises a clinical concern, it collects the relevant detail and escalates to your on-call person or the emergency instruction you set. Booking is administrative, and clinical judgement stays with your clinicians.
Is patient data sent overseas?
Your portal, transcripts, and structured call records sit in our Sydney data centre. The live audio of the call is processed offshore in real time. We are upfront about that split rather than claiming everything stays in Australia. The agent also collects the bare minimum a booking needs, so there is less sensitive data in play.
Does HIPAA apply to my New Zealand or Australian clinic?
No. HIPAA is United States law and has no force in New Zealand or Australia. Your obligations come from the Health Information Privacy Code 2020 in New Zealand, or the Australian Privacy Principles in Australia. Any vendor waving HIPAA at you is quoting the wrong country.
How fast can after-hours cover go live?
A focused after-hours build can go live quickly, because the scope is narrow. We start with evening and weekend overflow only, wire in your availability and escalation rules, and you review the morning summaries. Once you trust the bookings, you extend the same agent to daytime cover.
What happens on a genuine emergency call at 2am?
The agent recognises the urgent trigger you defined and gives the emergency instruction, such as calling 111 or 000. It then routes to your on-call line. It does not attempt to book or assess. The agent is tuned to escalate generously, so a borderline call still reaches a person.
Leonardo Garcia-Curtis
Founder & CEO at Waboom AI. Building voice AI agents that convert.
Ready to Build Your AI Voice Agent?
Let's discuss how Waboom AI can help automate your customer conversations.
Book a Free Demo

