Is an AI receptionist safe for a NZ or AU medical practice? Healthcare voice AI compliance is the right question, and the honest answer is yes, with conditions you can actually check. A clinic in Hamilton runs an AI receptionist on Tuesday morning. It books patients, takes messages, and answers the phone at 7pm when nobody is at the desk.
The patient data it touches is some of the most sensitive a business holds. So safe means two things. The rules that apply to that data, and where that data physically lives.
This piece walks both. We name the laws that bind you, we show where the records sit, and we list what to confirm before any agent touches a patient file.
The American badge does not bind your clinic. Two local frameworks do.
Is an AI receptionist safe for a NZ or AU medical practice?
Yes, when the agent is built for the rules that govern health information in your country and you confirm where the data lives. An AI receptionist is software handling personal data, and the same privacy law that covers your front-desk staff covers the agent. The question is not whether AI is allowed. It is whether your provider has answered the right ones.
A medical practice already runs phones, a booking system, and a patient management system. The AI receptionist sits in that chain. It hears a name, a date of birth, sometimes a symptom. That is health information, and health information carries extra duties on both sides of the Tasman.
The trap is importing the wrong framework. Plenty of vendors wave around an American acronym and call it compliance. That acronym does not apply to you. Let us clear that up first, then walk the rules that actually do. Our approach to securing health calls answers each one in plain terms.
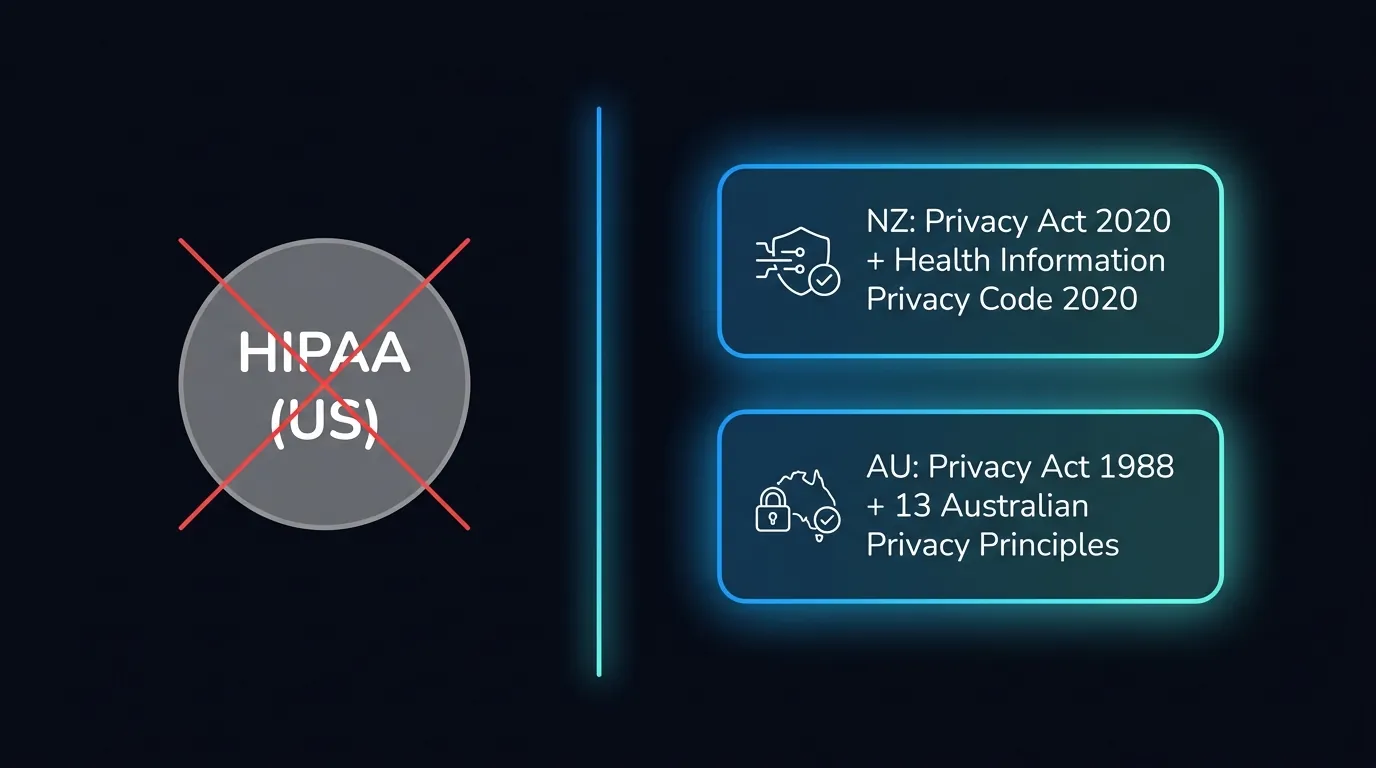
Why is HIPAA the wrong law, and what applies instead?
HIPAA is United States law. It does not apply to a New Zealand or Australian medical practice. A vendor selling you HIPAA compliance for a Christchurch clinic is selling a sticker for the wrong country. What applies in New Zealand is the Privacy Act 2020 and the Health Information Privacy Code 2020. In Australia it is the Privacy Act 1988 and the 13 Australian Privacy Principles.
HIPAA governs covered entities in the US health system. Your obligations live with the Office of the Privacy Commissioner in New Zealand and the OAIC in Australia. Those are the regulators who can ask you questions if a patient complains.
So when you assess an AI receptionist, ignore the American badge. Ask whether the provider has read the local code, and whether their answers reference the principles that bind you. The right framing is not whether the agent is fancy. It is whether the data handling maps to your duties. We unpack the wider picture in our guide to privacy across both countries.
What does the Health Information Privacy Code 2020 require?
In New Zealand the Health Information Privacy Code 2020 sets 13 rules for how health agencies collect, store, use, and disclose health information. It applies the moment your agent takes a patient name and a reason for calling. The big ones for an AI receptionist are purpose, security, retention, and access.
Collect only what you need for the booking or message. A receptionist does not need a full medical history to put a patient in a 9am slot. Store it securely, and keep it only as long as the clinical purpose requires. Let patients see and correct what is held about them.
Disclosure matters most. Health information should move only to people who need it for care or administration. So the agent should write to your patient management system, not scatter records across tools. You can read the full code at the New Zealand legislation site.
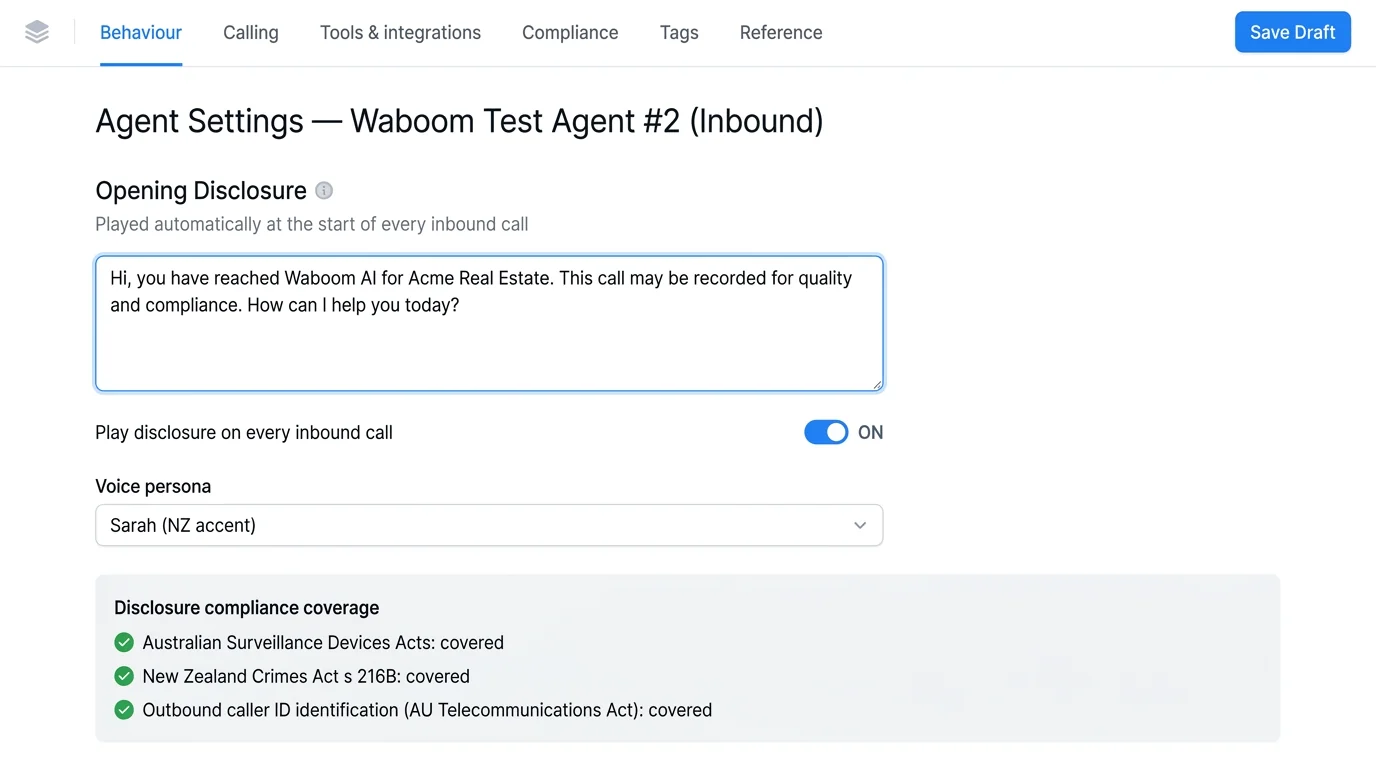
There is also a duty to be straight with the caller. We disclose on every single call that the patient is speaking with an AI. No pretending. That honesty is both a trust move and a compliance habit, and we cover it in our piece on telling callers they are speaking with an AI.
Want the data handling on one page?
Our healthcare security overview lays out what we collect, where it lives, and how long we keep it.
What do the Australian Privacy Principles require for health data?
In Australia health information is sensitive information under the Privacy Act 1988, and the 13 Australian Privacy Principles govern it. Sensitive information gets a higher bar than ordinary personal data. You generally need consent to collect it, you must secure it, and you must let people access and correct it.
APP 3 limits collection to what is reasonably necessary. APP 6 limits use and disclosure to the purpose you collected for. APP 11 demands reasonable security and deletion when no longer needed. The OAIC publishes guidance and can investigate complaints.
For an AI receptionist that means tight scope. Take the booking detail, write it where it belongs, and do not hoard recordings you never use. The full principles sit on the OAIC site. Australian government bodies write program, not programme, so match local spelling in patient-facing notices.

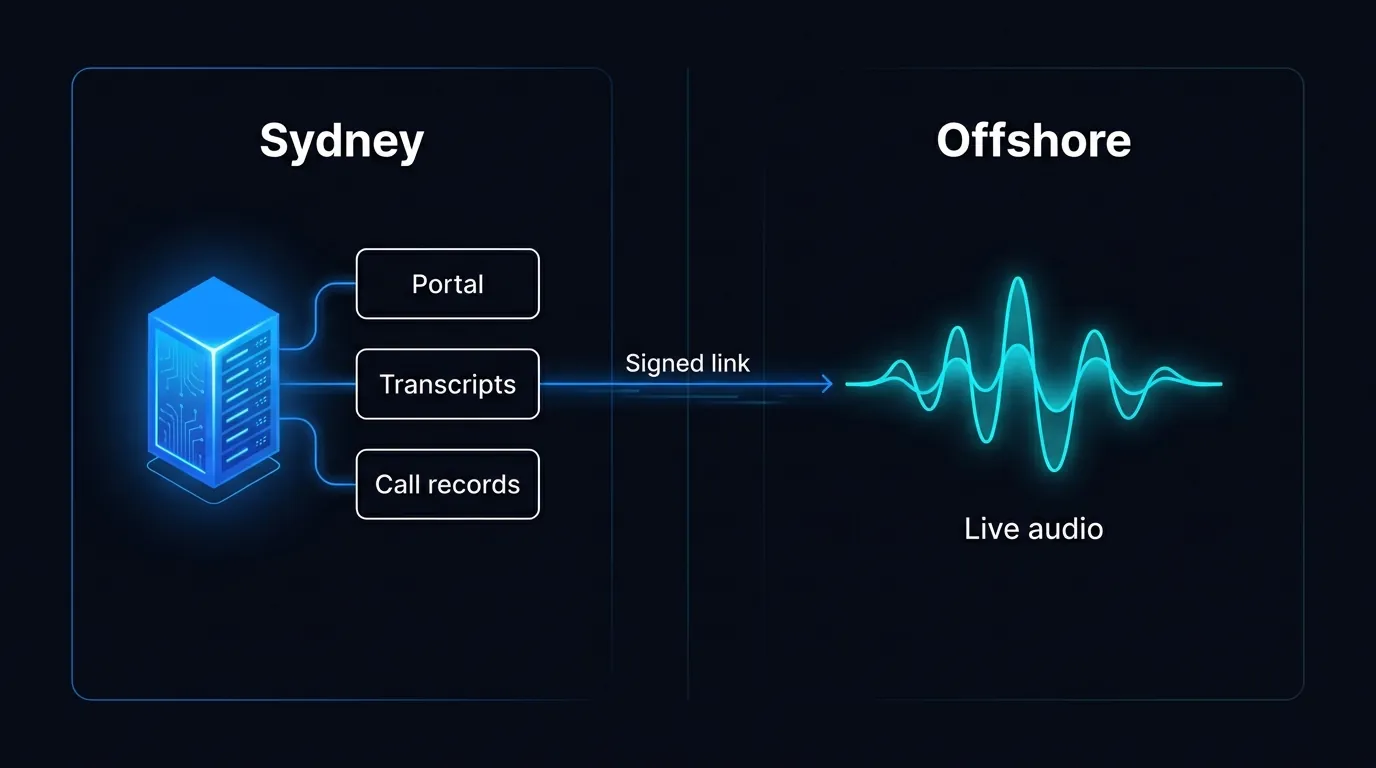
The honest residency split: records in Sydney, live audio processed offshore.
Where does patient call data actually live?
Here is the honest split most vendors skip. Our portal, transcripts, and structured call records sit on our Sydney servers. The live audio of the call is processed offshore while the conversation happens. We will not tell you all data stays in Australia, because that is not true and you would find out the hard way.
What this means in plain terms. The lasting record of a patient call, the part you query and report on, stays in Sydney. The moment-to-moment audio, the voice turning into text in real time, runs on infrastructure outside the country. Both legs are covered by the security duties above.
A clinic manager needs this on paper before go-live. Ask any provider exactly which data sits where, and get it in writing. If they cannot answer cleanly, that is your answer. We go deeper on storage choices in our note on keeping the data footprint small.
We also keep the footprint small on purpose. The less audio we retain, the less there is to protect. That is a buyer outcome, not a database lecture. Fewer copies of a patient voicemail means fewer ways it can ever leak.
What should a clinic confirm before an AI touches a patient record?
Confirm five things in writing before the agent goes near a patient record. Which law the provider builds to, where each type of data lives, what is collected, who can access it, and whether the AI discloses itself on every call. If any answer is vague, stop.
Run a short checklist with your provider.
This is the same diligence you would run on any new clinical supplier. The difference is the AI answers the phone at 7pm on a Friday, so the controls have to hold without a human watching. See how we fit a practice in our clinic walkthrough and our broader security overview.
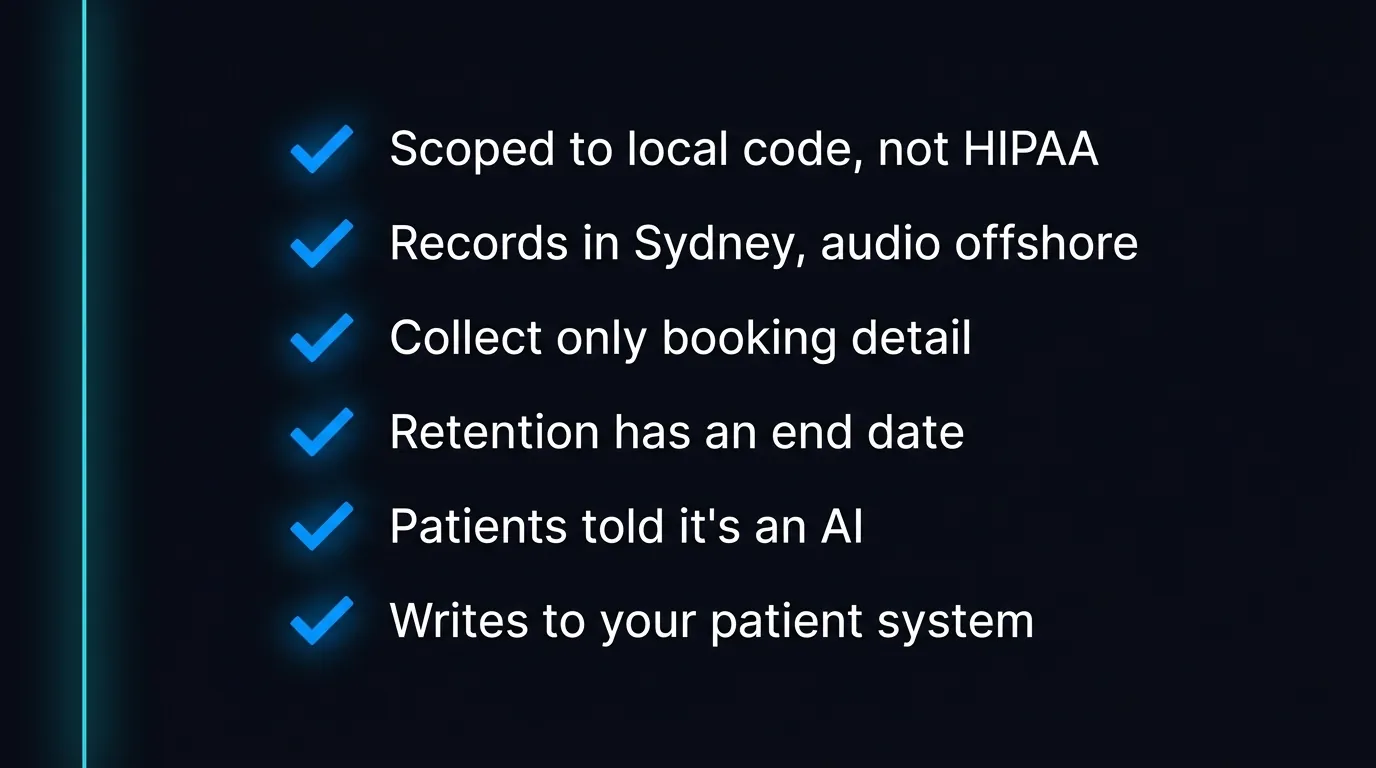
Six lines to confirm in writing before an agent touches a patient record.
Which patient calls should always go to a person?
Some calls should never sit with an AI. Clinical advice, a patient in distress, anything that sounds like an emergency, and complex triage all belong with a human. The agent should recognise these, say so, and hand off fast. Roughly a fifth of clinic calls need that human path, and the design has to assume it.
A patient ringing about chest pain does not want a booking. They want a person or an ambulance. So the agent is built to escalate, not to play doctor. We cover this line in our piece on why voice agents still hand off to people.
The economics still work. A NZ or AU part-time receptionist runs roughly 28 to 35 dollars an hour before KiwiSaver or super, ACC, and holiday pay. Our agent bills about 80 cents a minute, by the second, and an average answered call runs about 30 seconds, so close to 40 cents. The AI takes the volume so your people handle the calls that need a human.
That is the real pitch. Not replacing the receptionist. Covering the overflow and the after-hours block so no patient hits a dead line. The sensitive calls still reach someone who can help. See how this fits a clinic on our medical clinic page and our wider healthcare overview.
Ready to see it for your practice?
Walk through the data map and the human handoff on our healthcare voice agents page and we will show you exactly what a patient call leaves behind.
Frequently Asked Questions
Does HIPAA apply to my New Zealand or Australian clinic?
No. HIPAA is United States law for US health entities. A NZ clinic answers to the Privacy Act 2020 and the Health Information Privacy Code 2020. An Australian clinic answers to the Privacy Act 1988 and the 13 Australian Privacy Principles. Any vendor selling HIPAA compliance for your local practice is using the wrong framework, and you should ask why.
Where is my patient call data stored?
Our portal, transcripts, and structured call records sit on Sydney servers in Australia. The live audio of each call is processed offshore while the conversation is happening. We never claim all data stays in Australia, because it does not. Get the exact data map from any provider in writing before you let an agent touch a patient record.
Are patients told they are speaking with an AI?
Yes. We disclose on every single call that the caller is speaking with an AI. There is no pretending it is a human. This is both honest practice and a sensible compliance habit under New Zealand and Australian privacy expectations. It builds more trust than people expect when a clinic is upfront.
What patient information does the agent collect?
Only what the booking or message needs. A name, contact detail, reason for calling, and a preferred time. It does not gather a full medical history to put someone in a slot. Collection is scoped to the purpose, which is what both the Health Information Privacy Code and the Australian Privacy Principles require.
What does an AI receptionist cost a clinic?
About 80 cents a minute in NZD or AUD, billed by the second. An average answered call runs around 30 seconds, so roughly 40 cents. A one to two minute booking lands near one to two dollars. Compare that to a part-time receptionist at 28 to 35 dollars an hour before KiwiSaver or super, ACC, and holiday pay.
Which calls should still go to a human?
Clinical advice, distress, emergencies, and complex triage. The agent is built to spot these, tell the caller, and hand off fast rather than play doctor. Around a fifth of clinic calls need a human path, so the design assumes it. The AI carries the routine volume and after-hours overflow so your people handle what matters.
Leonardo Garcia-Curtis
Founder & CEO at Waboom AI. Building voice AI agents that convert.
Ready to Build Your AI Voice Agent?
Let's discuss how Waboom AI can help automate your customer conversations.
Book a Free Demo